

DFSV Training Implementation model

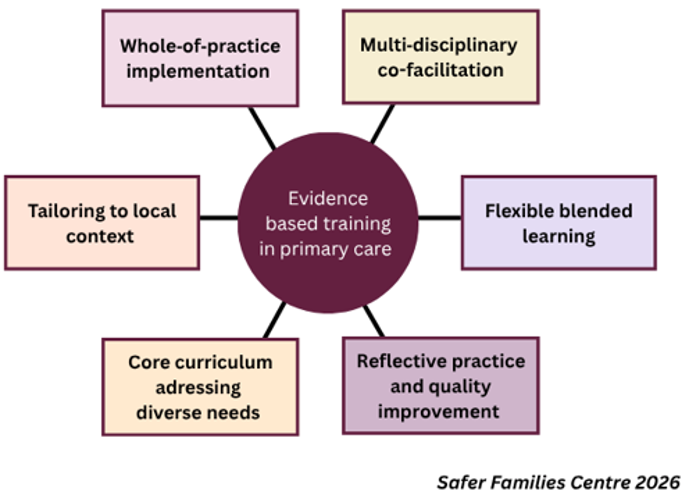
The model demonstrates the key elements of domestic, family and sexual violence (DFSV) training that supports sustained changes in practice. It incorporates recommendations developed by the Safer Families Centre on how to implement evidence-based training in primary care.
This model was developed by Safer Families Centre from a synthesis of findings from its DFSV training models and programs aiming to build the capacity of primary care to address DFSV and build greater cohesion across primary care, social care and family violence services (Sustainable Primary Care FV model, CATCH model, REAL model, The Readiness Program, Pathways to Safety, and our collaborations with Primary Health Networks).
Read further for key elements of the model and corresponding recommendations.
-
Whole‑of‑practice implementation approach to primary care training for domestic, family and sexual violence, and child sexual abuse.
Multidisciplinary co‑facilitation of training involving GP/Primary care nurse, DFV support worker and lived expertise facilitators.
Flexible, blended learning specific to role, learning preferences and current training level.
Core curriculum with consistent messaging and tools that can be adapted to address diverse workforce needs.
Training tailored to the local context to ensure cultural safety, clear referral pathways and appropriate supports.
Reflective practice and quality improvement using audit feedback and multidisciplinary case reflection sessions to drive improvement.
-
Whole‑of‑practice implementation
Obtain leadership support for all of staff involvement and appoint a DFV lead in each practice.
Expand training to include psychologists, social workers, allied health clinicians and local mental health teams to strengthen collaborative care.
Integrate system capacity building strategies such as practice readiness checklists, routine DFV processes, orientation for new‑staff induction, training refreshers and waiting room posters.
Embed clinical tools such as one-page referral pathway, screening prompts, safety plan and documentation templates.
Normalise peer discussions about DFSV cases to promote clinician wellbeing
Multidisciplinary co‑facilitation
Ensure co‑facilitation of training involves primary care clinicians, DFSV service staff and lived expertise facilitators to model collaborative care, clarify referral roles and integrate practical survivor-centred changes.
Provide support through facilitator check-in meetings to upskill, overcome challenges and ensure consistent delivery.
Ensure clear pre‑session briefings, facilitated reflection afterwards, and access to wellbeing supports or trainers.
Offer formal recognition, fair remuneration and mentoring pathways for Lived Expertise facilitators.
Flexible, blended learning
Offer brief role-specific modules for GPs, nurses, reception and managers, allied health, mental health including a mix of self‑paced e‑modules, webinars and in person workshops with role plays and practical exercises.
Keep training experiential and practice‑focused with interactive workshops, case studies, observed role‑play and opportunity for clinicians to practice with peer support.
Core curriculum addresses diverse needs
Define a core curriculum that covers respectful enquiry, first line response including safety assessment, documentation, referral pathways and legal duties, with elective modules for role‑specific needs.
Offer advanced modules for clinicians covering children exposed to DFSV and child sexual abuse, assessment and management of partners who use violence, sexual violence and reproductive coercion, suicide prevention in DFSV contexts, and technology‑facilitated abuse.
Ensure cultural safety by including training co-designed with Aboriginal and Torres Strait Islander representatives and organisations, and racially minoritised and LGBTQI+ communities.
Tailoring to local context
Trainers / facilitators to engage with practice to understand and determine practice and community needs.
Tailor content to local context by maintaining up‑to‑date resources and referral pathways, DFSV service contacts, and translated patient leaflets.
Embed templates and prompts into practice software and HealthPathways links for easy access during consultations.
Reflective practice and quality improvement
Implement clinical audits to monitor key indicators, including DFSV enquiry rates, documentation of safety plans, referrals, and follow-up care.
Use audit findings to support reflective practice, identify opportunities for improvement, and inform updates to training, clinical tools, and practice workflows.
Facilitate regular multidisciplinary case reflection sessions to review complex cases, discuss challenges, share learning, and consider improvements to clinical practice (including collaboration between general practices and specialist DFSV service providers).
Encourage structured reflection on individual and team experiences managing DFV presentations as part of ongoing continuing professional development and quality improvement.